
A penile fracture is a rare but serious urologic emergency that occurs when the fibrous tissue surrounding the erectile chambers of the penis (tunica albuginea) tears. Despite the term “fracture,” the penis does not contain a bone. Instead, this injury refers to a rupture of the erectile tissue during an erection, usually caused by sudden bending or blunt trauma. Immediate medical attention is essential to prevent long-term complications such as erectile dysfunction, penile curvature, or urethral injury.
Anatomy of the Penis
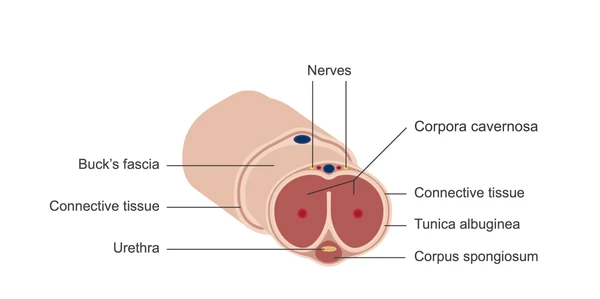
The penis contains three cylindrical structures:
- Corpora cavernosa – two dorsal (top) cylinders responsible for most of the erection.
- Corpus spongiosum – a ventral (bottom) cylinder that surrounds the urethra.
- Tunica albuginea – a strong fibrous layer that surrounds the corpora cavernosa, maintaining rigidity during an erection.
During sexual arousal, blood fills the corpora cavernosa and corpus spongiosum, causing the penis to enlarge and become rigid. If excessive force bends the erect penis, the tunica albuginea can tear, resulting in a penile fracture.
Causes and Mechanisms
How Does a Penile Fracture Occur?
A penile fracture typically occurs when the penis is erect and undergoes sudden, forceful bending or trauma. Common scenarios include:
- Sexual intercourse: Especially when the penis slips out of the partner and strikes the pelvic bone or perineum. Certain positions, such as when the partner is on top, have a higher risk.
- Energetic masturbation: Vigorous or rough handling can bend the erect penis.
- Unintentional trauma: Falls, rolling over in bed, or hitting the penis against walls or doors.
- Taqaandan: A cultural practice of forcefully bending the penis to reduce an erection, more common in the Middle East and Central Asia.
Men under 40, who tend to be more sexually active, are at greater risk.
Symptoms of Penile Fracture
A penile fracture usually presents with sudden and intense symptoms:
- A popping or cracking sound during the injury.
- Immediate loss of erection.
- Severe pain and discomfort.
- Rapid swelling and bruising (often forming a “eggplant-like” appearance).
- Penile deformity or curvature.
- Blood in the urine or at the tip of the penis (if the urethra is injured).
- Difficulty urinating.
⚠️ Even if there is no audible sound, the presence of rapid swelling, severe pain, and deformity should prompt urgent medical attention.
Diagnosis
Clinical Examination
A urologist can often diagnose penile fracture based on:
- Patient history (injury during erection, sound, sudden pain).
- Physical examination (swelling, bruising, curvature, hematoma).
Imaging Tests
In unclear cases, imaging may be used:
- Ultrasound: Can detect tunica albuginea tears and associated hematoma.
- MRI: Provides detailed images of soft tissue when ultrasound is inconclusive.
- Retrograde urethrogram: Assesses possible urethral injury, especially if blood is present in urine.
Treatment and Management
Surgery – The Gold Standard
Immediate surgical repair is the recommended treatment for penile fractures:
- A small incision is made at the base or around the fracture site.
- Hematomas are evacuated.
- The torn tunica albuginea is repaired using absorbable sutures.
- Urethral injuries, if present, are repaired simultaneously.
Benefits of early surgery:
- Restores normal penile anatomy and function.
- Reduces risk of long-term erectile dysfunction.
- Minimizes the chance of permanent curvature (Peyronie’s-like deformity).
Without surgery, men risk erectile difficulties, persistent pain, penile curvature, and urethral complications.
Non-Surgical Management
Only in very minor, non-fracture injuries (bruising or superficial trauma):
- Ice packs to reduce swelling.
- NSAIDs or acetaminophen for pain relief.
- Foley catheterization if necessary for urine drainage.
Non-surgical treatment is not recommended for true penile fractures.
Recovery and Postoperative Care
- Activity: Avoid sexual activity (including masturbation) for at least 4–6 weeks.
- Follow-up: Regular visits to monitor healing and detect complications.
- Pain and swelling: Usually resolve in 2–3 weeks.
- Full erectile function: Typically returns within 3–6 months if surgery is timely.
Complications may include:
- Penile curvature (10–30% of cases, usually mild).
- Painful erections.
- Erectile dysfunction (rare with timely repair).
- Fistula or weakened tissue in severe cases.
Prevention
- Avoid intentional bending of the erect penis.
- Use lubrication during sexual activity to reduce friction.
- Be cautious with sexual positions where control over the penis is limited.
- Older men may use medications to improve erections and reduce unexpected bending:
- Sildenafil (Viagra®)
- Tadalafil (Cialis®)
- Vardenafil (Levitra®)
- Avanafil (Stendra®)
Prognosis
With prompt surgical intervention, the prognosis is excellent:
- Success rate of surgery > 90%.
- Most men regain normal sexual function.
- Early repair significantly reduces risk of long-term complications.
When to Seek Immediate Medical Care
Go to the nearest emergency room if:
- You hear a popping or cracking sound during an erection.
- Experience sudden severe pain, swelling, or penile deformity.
- Notice blood in urine or difficulty urinating.
- Have ongoing or worsening pain after injury.
Even delayed treatment is better than no treatment, especially if symptoms persist.
Frequently Asked Questions
1. Can a penile fracture heal on its own?
No. Surgery is required to restore erectile function and prevent permanent curvature.
2. Can I have sex after penile fracture repair?
Sexual activity is typically resumed after 4–6 weeks, depending on the surgeon’s guidance.
3. Does penile fracture affect fertility?
Directly, no. But urethral damage or severe complications can indirectly affect semen passage.
4. How long does recovery take?
Pain and swelling usually resolve within 2–3 weeks, and full sexual function may return in 3–6 months.
5. Are there long-term risks after surgery?
Some men may develop mild curvature or occasional pain during erections, but serious complications are uncommon with timely repair.